

What comes to your mind when you think about a woman giving birth? Some may describe it as beautiful, a miracle, and a rite of passage. Others may think of pain, fear, and discomfort. Labor and delivery are not easy feats. It is called labor after all because it is a lot of work! In this section, you’ll learn more about the various approaches to childbirth as well as the actual process.
Childbirth
Approaches to Childbirth
Prepared childbirth refers to being not only physically in good condition to help provide a healthy environment for the baby to develop, but also helping a couple to prepare to accept their new roles as parents and to get information and training that will assist them for delivery and life with the baby as much as possible. The more a couple can learn about childbirth and the newborn, the better prepared they will be for the adjustment they must make to a new life. Nothing can prepare a couple for this completely. Once a couple finds that they are to have a child, they begin to conjure up images of what they think the experience will involve. Once the child is born, they must reconcile those images with reality (Galinsky, 1987). Knowing more of what to expect does help them in forming more realistic images thus making the adjustment easier. Let’s explore some of the methods of prepared childbirth.
HypnoBirthing
Grantley Dick-Read was an English obstetrician and pioneer of prepared childbirth in the 1930s. In his book Childbirth Without Fear, he suggests that the fear of childbirth increases tension and makes the process of childbearing more painful. He believed that if mothers were educated, the fear and tension would be reduced and the need for medication could frequently be eliminated. The Dick-Read method emphasized the use of relaxation and proper breathing with contractions as well as family support and education. Today this method is known as the Mongan Method or HypnoBirthing. Women using this method report feeling like they are lost in a daydream, but are focused and in control.
The Lamaze Method
This method originated in Russia and was brought to the United States in the 1950s by Fernand Lamaze. The emphasis of this method is on teaching the woman to be in control in the process of delivery. It includes learning muscle relaxation, breathing through contractions, having a focal point (usually a picture to look at) during contractions, and having a support person who goes through the training process with the mother and serves as a coach during delivery. The Lamaze Method is still the most commonly taught method in the U.S. today.
The Bradley Method
This method originated in the late 1940s and helps women deliver naturally, with few or no drugs. There are a series of courses that emphasize excellent nutrition and exercise, relaxation techniques to manage pain, and the involvement of the partner as a coach. Parents-to-be are taught to be knowledgeable consumers of birth services and to take responsibility in making informed decisions regarding procedures, attendants, and the birthplace. In turn, this will lead to keeping mothers healthy and low-risk in order to avoid complications that may lead to medical intervention.
Nurse-Midwives
Historically in the United States, most babies were born under the care of lay midwives. In the 1920s, middle-class women were increasingly using doctors to assist with childbirth but rural women were still being assisted by lay midwives. The nursing profession began educating nurse-midwives to assist these women. Nurse-midwives continued to assist most rural women with delivery until the 1970s and 1980s when their growth is thought to have posed a threat to the medical profession (Weitz, 2007). Women who are at low risk for birth complications can successfully deliver under the care of nurse-midwives. Some hospitals give privileges to nurse-midwives to deliver there. They may also deliver babies at home or in birthing centers.
Home Birth
Because one out of every 20 births involve a complication, most medical professionals recommend that delivery take place in a hospital. However, some couples choose to have their baby at home. About 1 percent of births occur outside of a hospital in the United States. Two-thirds of these are home births and more than half of these are assisted by midwives. In the United States, women who have had previous children, who are over 25 and who are white are most likely to not give birth in a hospital (MacDorman et al., 2010).
Birthing Centers
A birthing center presents a more home-like environment than a hospital labor ward, typically with more options during labor: food/drink, music, and the attendance of family and friends if desired. Other characteristics can also include non-institutional furniture such as queen-sized beds, large enough for both mother and father, and perhaps birthing tubs or showers for water births. The decor is meant to emphasize the normality of birth. In a birth center, women are free to act more spontaneously during their birth, such as squatting, walking, or performing other postures that assist in labor. Active birth is encouraged. The length of stay after birth is shorter at a birth center; sometimes just 6 hours after birth the mother and infant can go home. One-third of out-of-hospital births occur in freestanding clinics, birthing centers, or physician’s offices, or other locations.
Water Birth
Laboring and/or giving birth in a warm tub of water can help a woman relax. The buoyancy of the water can help alleviate discomfort and pressure for the mother. Many hospitals have birthing tubs that allow women to labor in them. However, only some hospitals allow for birth to take place in the water. Some believe that water birth gives a more calm and tranquil transition for the baby from the womb. Water births are more common to occur at home or in birthing centers.
Hospital Birth
Most births in the U.S. occur in hospitals. Mothers have the choice to have a medicated or unmedicated delivery. Some women do fine with “natural methods” of pain relief alone. Many women blend “natural methods” with medications and medical interventions that relieve pain. Building a positive outlook on childbirth and managing fear may also help some women cope with the pain. Labor pain is not like pain due to illness or injury. Instead, it is caused by contractions of the uterus that are pushing the baby down and out of the birth canal. In other words, labor pain has a purpose.
The most common pain relief method used during labor and delivery is an epidural. An epidural is a procedure that involves placing a tube into the lower back, into a small space outside the spinal cord. Small doses of medicine can be given through the tube as needed throughout labor. With an epidural, pain relief starts 10 to 20 minutes after the medicine has been given. The degree of numbness felt can be adjusted. An epidural can prolong the first and second stages of labor. If given late in labor or if too much medicine is used, it might be hard to push when the time comes.
Another form of pharmacologic pain relief available for laboring mothers is inhaled nitrous oxide. This is typically a 50/50 mixture of nitrous oxide with air that is an inhaled analgesic and anesthetic. Nitrous oxide has been used for pain management in childbirth since the late 1800s. The use of inhaled analgesia is commonly used in the UK, Finland, Australia, Singapore, and New Zealand, and is gaining in popularity in the United States.
The Process of Delivery
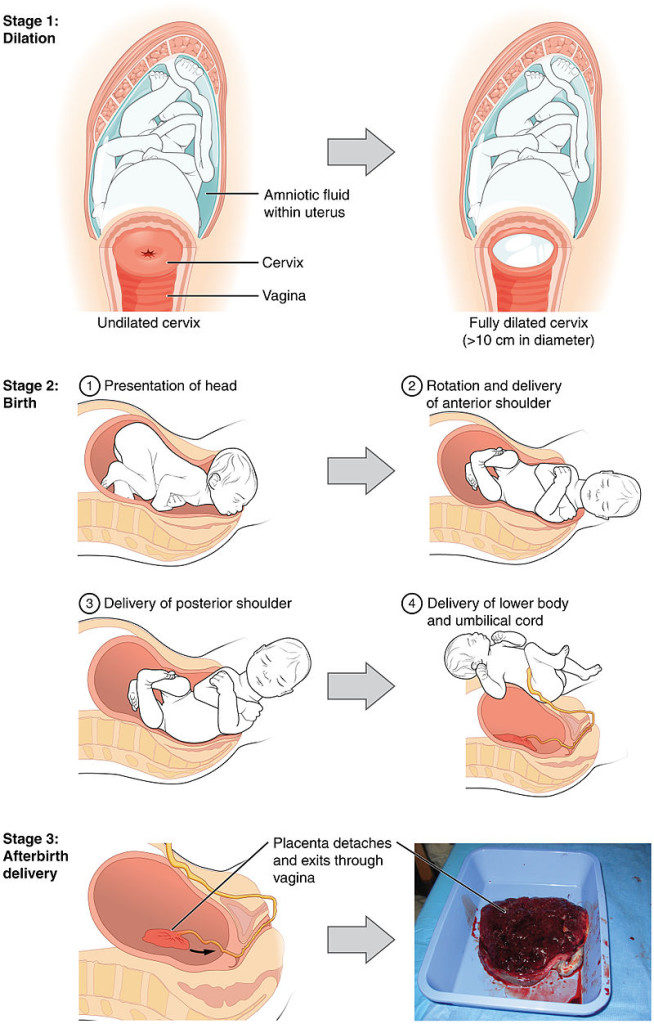
The first stage of labor is typically the longest. The first stage of labor begins with uterine contractions that may initially last about 30 seconds and be spaced 15 to 20 minutes apart. These increase in duration and frequency to more than a minute in length and about 3 to 4 minutes apart. Typically, doctors advise that they should be called when contractions are coming about every 5 minutes. Some women experience false labor or Braxton-Hicks contractions, especially with the first child. These may come and go. They tend to diminish when the mother begins walking around. Real labor pains tend to increase with walking.
During this stage, the cervix or opening to the uterus dilates to 10 centimeters (just under 4 inches). This may take around 12-16 hours for first children or about 6-9 hours for women who have previously given birth. It takes one in nine women over 24 hours to dilate completely. Labor may also begin with a discharge of blood or amniotic fluid. If the amniotic sack breaks, which happens for one out of eight pregnancies, labor will be induced if necessary to reduce the risk of infection.
The second stage involves the passage of the baby through the birth canal. This stage takes about 10-40 minutes. Contractions usually come about every 2-3 minutes. The mother pushes and relaxes as directed by the medical staff. Normally the head is delivered first. The baby is then rotated so that one shoulder can come through and then the other shoulder. The rest of the baby quickly passes through. The baby’s mouth and nose are suctioned out. The umbilical cord is clamped and cut.
The third stage is relatively painless in comparison to the other stages. During this stage, the placenta, or afterbirth is delivered. This typically occurs within 20 minutes after the delivery of the baby. If tearing of the vagina occurred during birth, the tear may be stitched at this time.
Cesarean Section
Cesarean section, also known as C-section, or cesarean delivery, is the use of surgery to deliver babies. A cesarean section is often necessary when a vaginal delivery would put the baby or mother at risk. This may include obstructed labor, twin pregnancy, high blood pressure in the mother, breech birth, or problems with the placenta or umbilical cord. Cesarean delivery may be performed based upon the shape of the mother’s pelvis or history of a previous C-section. A trial of vaginal birth after a C-section may be possible. The World Health Organization recommends that cesarean section be performed only when medically necessary. Some C-sections are performed without a medical reason, upon request by someone, usually the mother.
Newborn Assessment and Risks
Complications of the Newborn
Assessing the Neonate
There are several ways to assess the condition of the newborn. The most widely used tool is the Neonatal Behavioral Assessment Scale (NBAS) developed by T. Berry Brazelton. This tool has been used around the world to help parents get to know their infants and to make comparisons of infants in different cultures (Brazelton & Nugent, 1995). The baby’s motor development, muscle tone, and stress response are assessed.
The Appearance, Pulse, Grimace, Activity, and Respiration (APGAR) test is conducted at one minute and five minutes after birth. This is a very quick way to assess the newborn’s overall condition. Five measures are assessed: the heart rate, respiration, muscle tone (quickly assessed by a skilled nurse when the baby is handed to them or by touching the baby’s palm), reflex response (the Babinski reflex is tested), and color. A score of 0 to 2 is given on each feature examined. An APGAR of 5 or less is cause for concern. The second APGAR should indicate improvement with a higher score.
Low Birth Weight
We have discussed a number of teratogens associated with a low birth weight such as cocaine, tobacco, etc. A child is considered to have a low birth weight if they weigh less than 5.8 pounds (2500 grams). About 8.17 percent of babies born in the United States are of low birth weight and 1.4 percent are born with very low birth weight. A low birth weight baby has difficulty maintaining adequate body temperature because it lacks the fat that would otherwise provide insulation. Such a baby is also at more risk of infection. And 67 percent of these babies are also preterm which can make them more at risk for a respiratory infection. Very low birth weight babies (2 pounds or less) have an increased risk of developing cerebral palsy. Many causes of low birth weight are preventable with proper prenatal care.
Premature Birth
A child might also have a low birth weight if it is born at less than 37 weeks gestation (which qualifies it as a preterm baby). In 2016, 9.85 percent of babies born in the U.S. were preterm. Early birth can be triggered by anything that disrupts the mother’s system. For instance, vaginal infections or gum disease can actually lead to premature birth because such infection causes the mother to release anti-inflammatory chemicals which, in turn, can trigger contractions. Smoking and the use of other teratogens can also lead to preterm birth.
Anoxia and Hypoxia
One of the leading causes of infant brain damage is lack of oxygen shortly after birth. Hypoxia occurs when the infant is deprived of an adequate amount of oxygen, leading to mild to moderate brain damage. Apoxia occurs when the infant undergoes a total lack of oxygen, which can lead to severe brain damage. This lack of oxygen is typically caused by umbilical cord problems, birth canal problems, blocked airways, and placenta abruption. Both hypoxia and anoxia can lead to cerebral palsy and a host of other medical disorders.